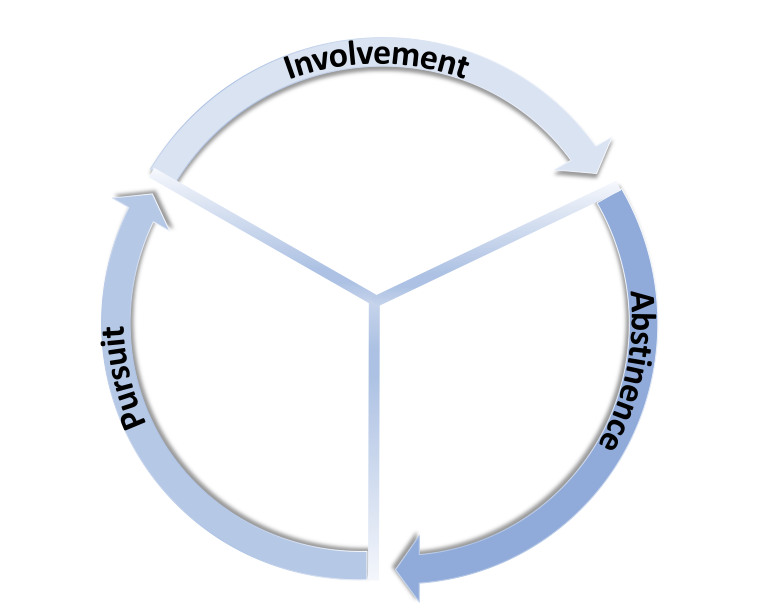
Addiction is a bio-psycho-social-spiritual disorder that is characterized by three discrete behavioral phases:
1) pursuit – actively seeking involvement with a substance or activity (e.g., drug addict stealing/selling property to get money for drugs; sex addict “cruising” in search of someone to “act out” with). Pursuit is quintessentially goal-directed behavior, in that it is directed toward some specific end (i.e., feeling good, feeling better, performing good/better).
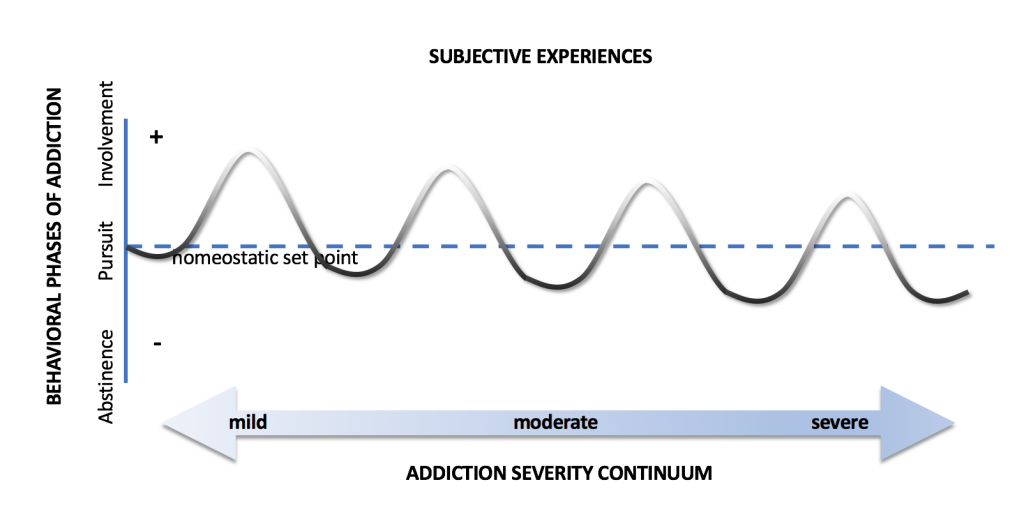
2) involvement – actively consuming a drug or engaging in an activity (e.g., alcoholic imbibing; gambling addict betting; sex addict “acting out”). The behavior of involvement is usually associated with positive experiences, which are described below. In general, the behavior of active involvement sets the cascade of addictive behaviors in motion. This is the phase that is accompanied by the experience of “reward,” which can reinforce the behavior. In the earliest stages of use, before addiction will have taken hold, one may or may not be able to regulate or moderate his/her involvement. However, during the later stages, once full-blown addiction has developed, one will generally be unable to control the amount, duration, or frequency of involvement. In recovery parlance, this is described as the phenomenon of craving, wherein “Once you start, you can’t stop.” Hence, there is rapid oscillation between the pursuit and involvement phases. At this point, one experiences an acute loss-of-control over behavior.
3) abstinence – There are effectively two types of abstinence: passive and active. Paradoxically, abstinence, that is, not doing something, is nevertheless constitutive of addictive behavior insofar as it tends to follow involvement, and usually represents a phase transition back into pursuit. Passive abstinence refers to the incidental intervals between episodes of active involvement, whereas active abstinence, for an addict desiring to refrain from involvement, refers to intentional cessation of involvement to avoid attendant consequences or to attain the benefits of abstention. Passive abstinence may be intrinsically motivated, as it may follow loss of consciousness, loss of interest in involvement (i.e., hangover), lack of resources (e.g., money, drugs). Alternatively, passive abstinence may be extrinsically motivated, in that it may follow external constraints placed on the individual (e.g., hospitalization, incarceration). On the other hand, active abstinence represents a potential transition into recovery, which I describe here.
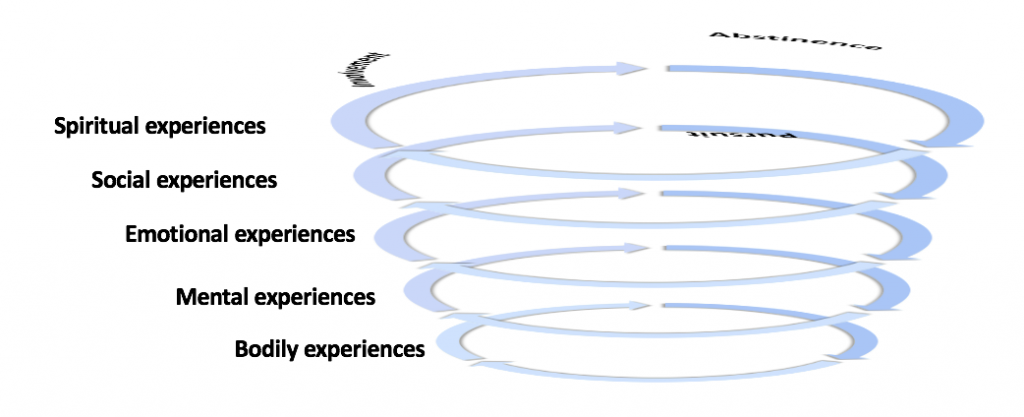
From a behavioral standpoint, the experience of addiction can be understood as a dynamic cycling between these three phases. Importantly, each of these three phases is accompanied by a variety of corresponding bodily, psychological (i.e., mental and emotional), social, and spiritual experiences, which I describe below. Hence, the behaviors that characterize addiction are objectives correlates of multidimensional subjective experiences.